.png)
Skin Barrier's Role in Pigmentation Control
- chevonne stewart
- Jul 3
- 8 min read


The skin barrier is the primary regulator of pigmentation by maintaining skin integrity and preventing the inflammation that triggers excess melanin production. When your barrier is intact, it limits transepidermal water loss (TEWL), blocks irritants, and keeps melanocytes calm. When it breaks down, inflammatory signals flood the skin and activate tyrosinase, the enzyme that drives melanin synthesis. Understanding the role of skin barrier in pigmentation control means recognizing that ceramides, niacinamide, and centella asiatica are not just moisturizing ingredients. They are the foundation of any effective pigmentation strategy.
What is the role of skin barrier in pigmentation control?
The skin barrier is a layered structure built from corneocytes and lipids, often described using the “brick and mortar” model. Corneocytes are the bricks, and a lipid matrix of ceramides, cholesterol, and fatty acids forms the mortar. This architecture physically blocks UV radiation, pollutants, and microbes from reaching the deeper layers where melanocytes live. When the mortar weakens, those triggers reach melanocytes directly, and pigment production rises.

TEWL in intact skin sits at approximately 300–400 mL per day. That number matters because elevated TEWL signals a leaky barrier, which correlates directly with chronic low-grade inflammation. Inflammation is the single most reliable driver of melanocyte overstimulation. A barrier that holds moisture in also holds inflammatory cascades out.
The three key lipids that maintain barrier integrity are:
Ceramides: Make up roughly half the lipid matrix and seal intercellular spaces between corneocytes.
Cholesterol: Regulates lipid fluidity and supports barrier flexibility across temperature changes.
Fatty acids: Work alongside ceramides to maintain the acidic pH of the skin surface, which keeps harmful bacteria and enzymes from degrading the barrier.
Each of these lipids plays a direct role in pigmentation regulation because their absence creates the inflammatory conditions that stimulate melanin synthesis.
Barrier Component | Function | Pigmentation Impact |
Ceramides | Seal intercellular spaces | Prevent irritant-driven melanocyte activation |
Cholesterol | Maintain lipid fluidity | Support barrier flexibility and UV defense |
Fatty acids | Regulate surface pH | Limit inflammatory enzyme activity |
Corneocytes | Physical block against irritants | Reduce UV and pollutant penetration |
How does a compromised skin barrier lead to increased pigmentation?
A damaged barrier does not just let moisture escape. It opens a direct pathway for irritants, UV radiation, and microbial fragments to reach the living layers of skin. Once those triggers arrive, the immune system responds with cytokines and prostaglandins, two classes of inflammatory mediators that signal melanocytes to produce more melanin. This is the biochemical root of post-inflammatory hyperpigmentation (PIH).
Barrier compromise activates melanocytes even when the original insult is minor. A small scratch, a harsh cleanser, or a single sunburn can set off a chain reaction that leaves a dark mark for months. Skin of color is especially vulnerable because melanocytes in deeper skin tones are primed to respond more intensely to inflammatory signals.
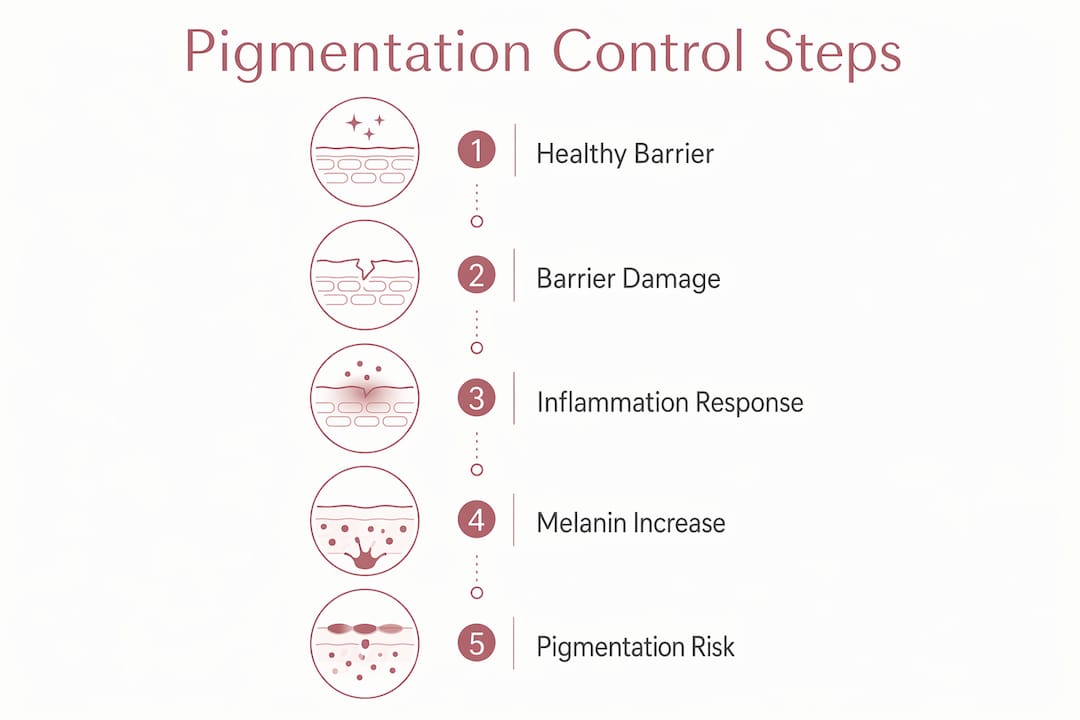
The cycle looks like this:
Barrier disruption raises TEWL and allows irritants in.
Irritants trigger cytokine and prostaglandin release.
Inflammatory mediators activate tyrosinase.
Tyrosinase converts tyrosine into melanin.
Melanin deposits unevenly, creating dark spots or patches.
Ongoing barrier weakness keeps the cycle running.
Pigmentation is not just melanin overproduction. It is also a failure of clearance and a reaction to ongoing barrier damage. A compromised barrier perpetuates continuous melanocyte activation, which is why treating the pigment alone, without addressing the barrier, rarely produces lasting results.
Pro Tip: If you notice that your dark spots return quickly after treatment, the barrier is likely still compromised. Focus on barrier repair for at least four weeks before reintroducing any brightening actives.
Which factors commonly damage the skin barrier and worsen pigmentation?
Several external and internal factors strip the lipid matrix and weaken the barrier. Knowing them helps you avoid the habits that keep pigmentation cycling back.
Environmental factors:
UV radiation degrades ceramides and triggers immediate inflammatory responses, increasing melanin production and photoaging.
Air pollution deposits particulate matter that generates free radicals, breaking down the lipid matrix over time.
Low humidity accelerates TEWL, thinning the hydration layer that supports barrier integrity.
Skincare habits that cause damage:
Over-cleansing with sulfate-heavy or alkaline cleansers strips the acidic mantle and removes protective lipids.
Overusing exfoliating acids or retinoids before the barrier is ready disrupts corneocyte cohesion.
Applying active brightening ingredients on a compromised barrier worsens irritation and can deepen pigmentation rather than fade it.
Inflammatory skin conditions:
Acne, eczema, and rosacea all involve barrier dysfunction as a core feature, not just a side effect.
Research on IL-4 and related cytokines shows that chronic inflammatory signaling degrades barrier proteins and sustains melanocyte activation long after the visible inflammation resolves.
Mechanical damage from picking, rubbing, or aggressive facial massage creates micro-tears that trigger localized PIH.
The most damaging pattern is treating pigmentation aggressively while ignoring the barrier. Harsh treatments create more inflammation, which creates more pigment, which prompts more aggressive treatment. Breaking that cycle requires stopping the inflammatory input first. You can read more about adjusting your skincare to avoid these triggers.
How can you repair the skin barrier to control pigmentation?
Barrier repair follows a clear sequence. You cannot effectively fade pigmentation on skin that is still inflamed and leaking. The stratum corneum turnover cycle takes approximately four weeks, which means you need at least that long to see measurable structural improvement before adding brightening actives.
Step-by-step barrier repair protocol:
Switch to a non-stripping cleanser. Use a low-pH, sulfate-free formula that cleans without removing protective lipids. Gel or cream cleansers with a pH of 4.5–5.5 preserve the acidic mantle.
Apply a ceramide-rich moisturizer immediately after cleansing. Ceramides, cholesterol, and fatty acids in a 3:1:1 ratio most closely replicate the natural lipid matrix. Apply while skin is still slightly damp to reduce TEWL.
Add niacinamide to your routine. Niacinamide strengthens the barrier by increasing ceramide synthesis and reduces melanin transfer from melanocytes to surrounding cells. It works on both barrier repair and pigmentation simultaneously.
Incorporate centella asiatica. This plant extract calms inflammatory signaling and supports collagen production in the dermis, reducing the inflammatory triggers that activate melanocytes.
Use hyaluronic acid as a hydration anchor. Hyaluronic acid draws water into the stratum corneum, reducing TEWL and supporting the environment in which lipid lamellae can rebuild.
Pause all exfoliating acids and retinoids for the first four weeks of barrier repair. Reintroduce them slowly, starting with the lowest effective concentration once the barrier shows signs of recovery.
Pro Tip: Signs that your barrier is recovering include less redness after washing, reduced sensitivity to products you previously tolerated, and a more even skin tone without new dark spots appearing. These changes typically emerge within two to four weeks of consistent barrier-focused care.
You can also support your skin with targeted ingredients. The Medicube AGE-R Vita K Cream combines Vitamin K with anti-inflammatory actives that complement a ceramide-focused barrier repair routine.
What role does inflammation-aware care play in pigmentation treatment?
Inflammation-aware skincare means sequencing your treatments so that barrier repair comes before brightening. Applying strong actives like hydroquinone, kojic acid, or high-concentration vitamin C on a compromised barrier does not accelerate results. It worsens irritation and deepens pigmentation by triggering more inflammatory mediators.
Barrier repair reduces reactive pigmentation and improves the efficacy of brightening treatments applied afterward. This is not a minor benefit. It is the difference between a treatment that works once and one that produces lasting results. Skin that has a healthy barrier tolerates active ingredients better, absorbs them more evenly, and responds with less rebound pigmentation.
Repairing the barrier first is not a delay in treatment. It is the treatment. Skin that cannot hold moisture or resist irritants will keep producing melanin regardless of what brightening actives you apply on top. Phasing care to prioritize barrier integrity is the most direct path to stable, long-term pigmentation control.
Post-inflammatory hyperpigmentation is strongly linked to barrier compromise, particularly in skin of color. Inflammation-aware care reduces the frequency and severity of PIH by removing the inflammatory trigger before it reaches melanocytes. Once the barrier is stable, brightening actives work faster and the results hold longer. You can explore pigmentation treatment options that integrate this phased approach.
Key Takeaways
A healthy, intact skin barrier is the most direct and reliable tool for long-term pigmentation control, because it prevents the inflammation that drives melanin overproduction.
Point | Details |
Barrier integrity controls melanin | An intact barrier limits TEWL and blocks inflammatory triggers that activate tyrosinase. |
Compromised barrier drives PIH | Barrier damage releases cytokines and prostaglandins that stimulate melanocytes and cause dark spots. |
Repair before brightening | Applying active ingredients on a damaged barrier worsens pigmentation; repair the barrier first over four weeks. |
Key repair ingredients | Ceramides, niacinamide, centella asiatica, and hyaluronic acid rebuild the lipid matrix and reduce inflammation. |
Inflammation-aware sequencing | Phasing treatments to prioritize barrier health reduces relapse and improves the efficacy of brightening actives. |
What I’ve learned after 15 years of treating pigmentation
Most people who come to me frustrated with their pigmentation have one thing in common. They have been treating the symptom, not the source. They have tried brightening serums, chemical peels, and laser treatments, and the spots keep coming back. When I look at their skin, the barrier is almost always compromised. It is red, reactive, and sensitive to products it should tolerate easily.
The uncomfortable truth about pigmentation is that it is often your skin’s defense response, not a cosmetic flaw. When the barrier is weak, your skin produces melanin to protect itself from the inflammation and UV exposure it can no longer block. Treating the pigment without fixing the barrier is like mopping the floor while the tap is still running.
What I tell every client is this: patience with barrier repair is not passive. It is the most active thing you can do for your skin. Four weeks of ceramide-rich moisturizers, gentle cleansers, and no harsh actives will do more for your long-term pigmentation than any aggressive treatment applied to a compromised skin surface.
The other misconception I see constantly is that professional treatments and barrier repair are separate tracks. They are not. The best results I have seen come from clients who pair professional treatments with a consistent, barrier-focused home routine. The treatments accelerate the process. The barrier work makes the results stick.
— chevonne
Fundamentalskin’s approach to barrier-focused pigmentation care
If you are ready to move beyond surface-level treatments, Fundamentalskin offers professional options designed around barrier integrity and pigmentation control.
The Larimedical Biomimetic Peel is a non-invasive treatment that supports barrier repair while addressing pigmentation, redness, and uneven skin tone. It works with your skin’s natural renewal process rather than against it, making it suitable for sensitive and pigmentation-prone skin. For clients who want to combine barrier recovery with light therapy, the Biomimetic Peel + LED Therapy offers a clinically guided session that reduces inflammation and supports pigment fading simultaneously. Chevonne tailors every treatment to your skin’s current barrier status, so you never receive an active treatment your skin is not ready for.
FAQ
What is the skin barrier’s main function in pigmentation?
The skin barrier limits transepidermal water loss and blocks irritants and UV radiation from reaching melanocytes. When the barrier is intact, melanocyte activation stays low and pigmentation remains stable.
Can a damaged skin barrier cause dark spots?
Yes. Barrier damage triggers cytokine and prostaglandin release, which activates tyrosinase and increases melanin production. This is the direct mechanism behind post-inflammatory hyperpigmentation.
How long does it take to repair the skin barrier?
The stratum corneum completes one turnover cycle in approximately four weeks. Consistent use of ceramide-rich moisturizers and gentle cleansers during this period produces measurable barrier improvement.
Should I stop using brightening serums while repairing my barrier?
Active brightening ingredients applied to a compromised barrier worsen irritation and can deepen pigmentation. Pause strong actives during the initial four-week repair phase, then reintroduce them gradually.
Which ingredients best support skin barrier repair for pigmentation control?
Ceramides, niacinamide, centella asiatica, and hyaluronic acid are the most clinically supported ingredients for barrier repair. Niacinamide also reduces melanin transfer, making it effective for both barrier function and pigmentation regulation simultaneously.
Recommended
Comments